Login

www.reeleak.com
Reeleak is an alternative to LiveGore, now you can surf and watch LiveGore content directly from Reeleak.
WARNING: UNCENSORED NEWS!
LiveGore is a reality news website which reports on real life events which are of the interest to the public. Includes videos relating to true crime that have been taken from across the world. Due to the graphic nature of materials found on Live Gore, access is restricted to adults only(18+). !!Please leave this website if you under that age!!Important Update!
Please join our telegram channel to get important updates related to this website.
Join now : https://t.me/+aI6AdrheUSlhYTNh/
New poll : https://t.me/c/2146536856/5/
New note : https://t.me/c/2146536856/7/
Join our telegram for news update!
https://t.me/+aI6AdrheUSlhYTNh/
Announcement Box
Please check our new announcement.
READ : https://t.me/livegoredotcom/37
ARE YOU OVER 18 YEARS OLD?
You must be 18 or older to enter this website.
By clicking "YES", you confirm that you are of legal age to view this content.
If you are under 18, please click "NO" to exit the site.
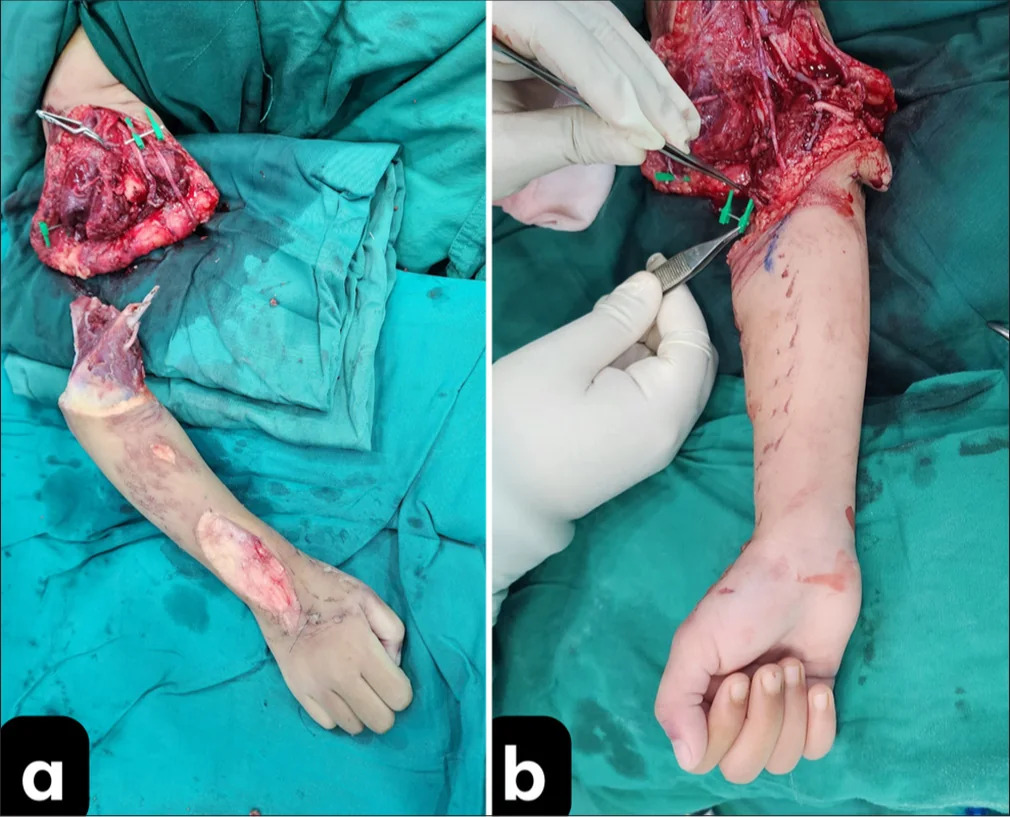
Fig 1: (a) Nerve anastomosis prep after completing vascular anastomosis; (b) right wrist in neutral position; and (c) full extension of the right wrist shows signs of nerve recovery
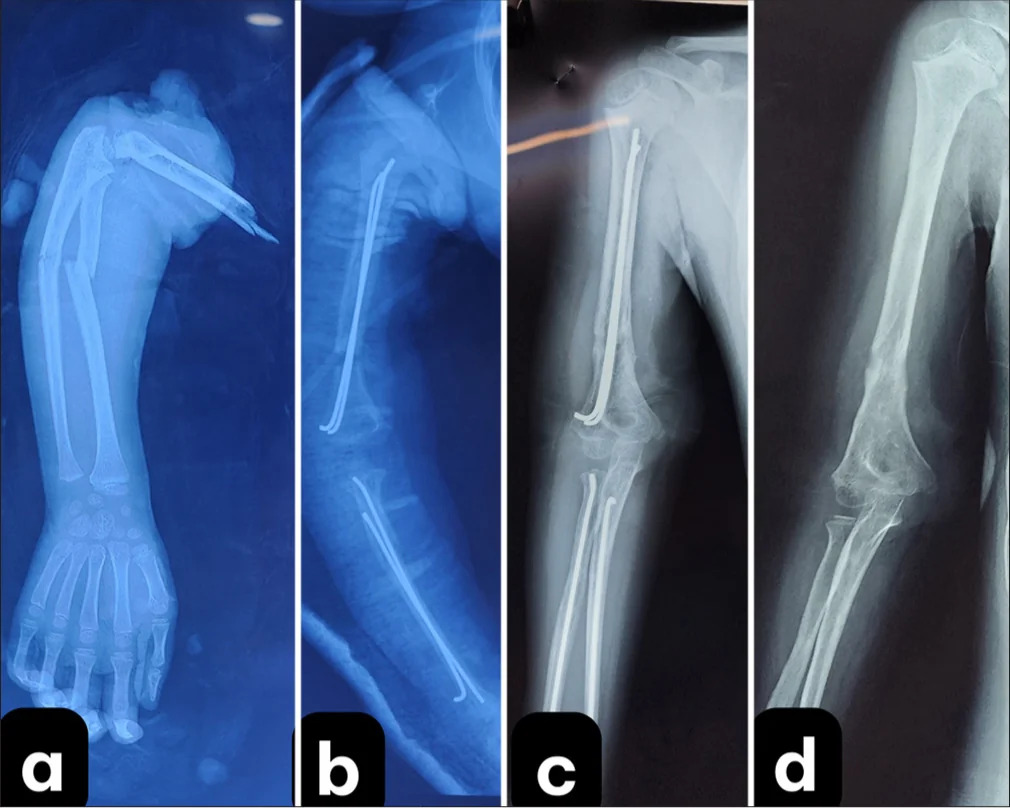
Fig 2: X-ray images before and after surgery.
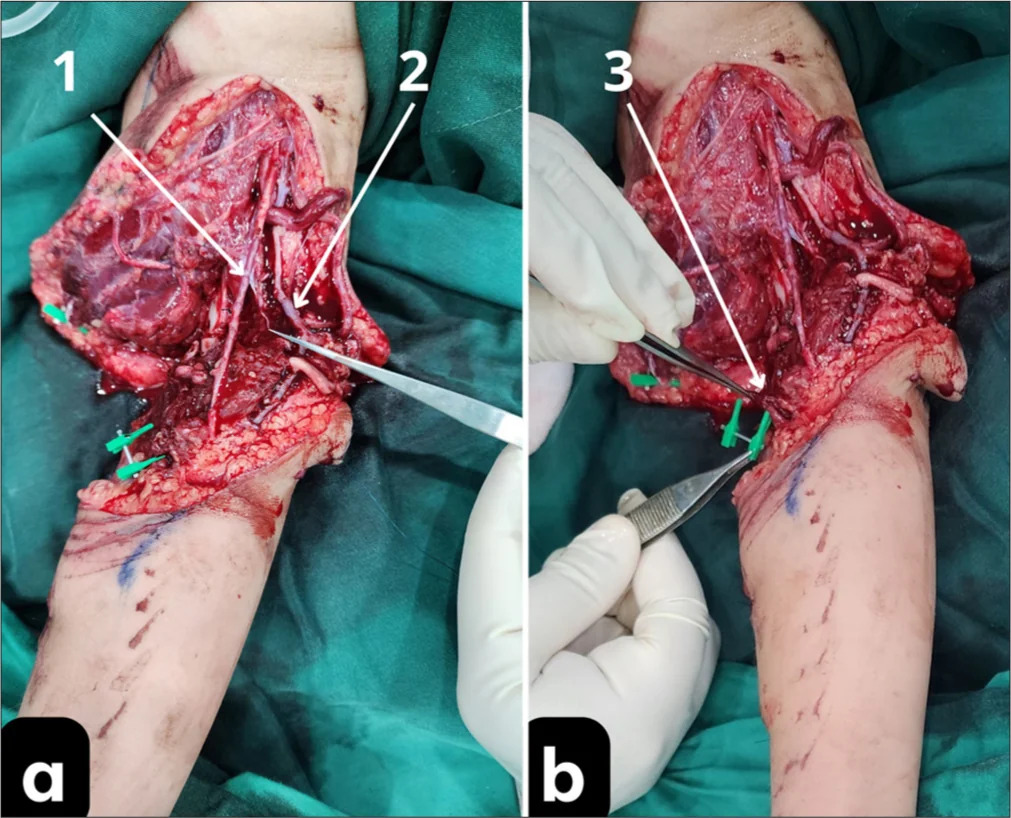
Fig 3: (a) Completion of one vein and one artery anastomosis, 1: patent artery, 2: patent vein; and (b) proceeding with the next vein anastomosis, 3: pre-marked location of the vein.
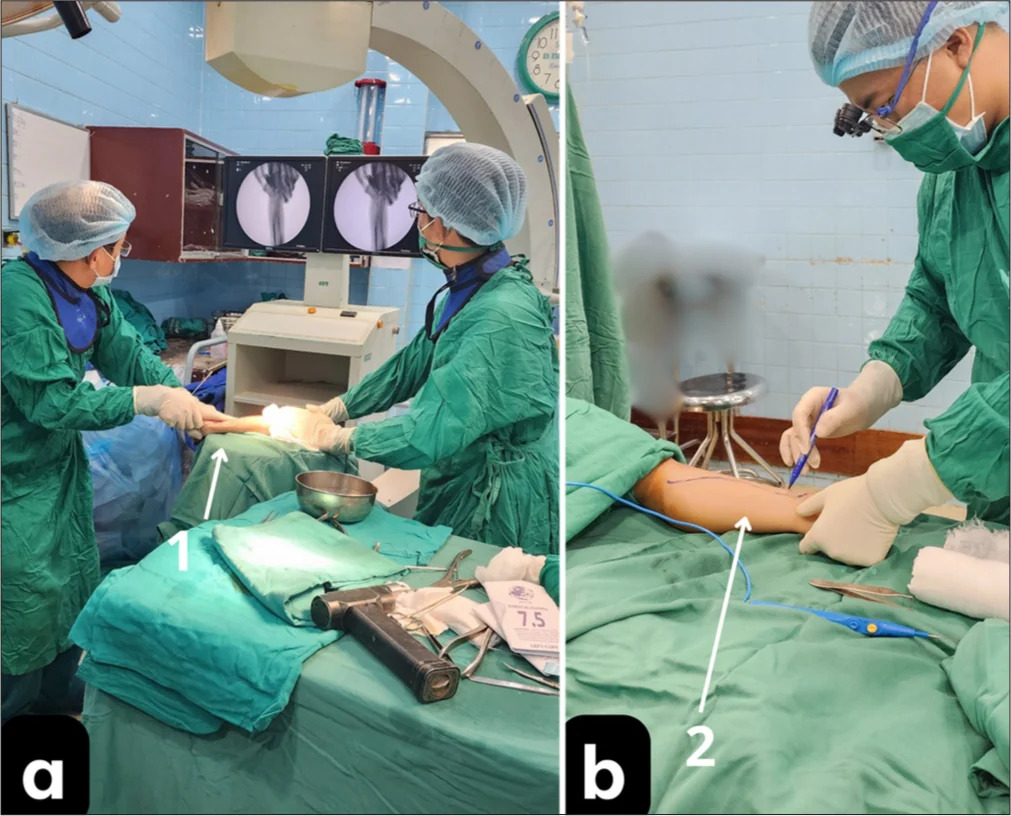
Fig 4: (a) forearm bone fixation with intramedullary nailing, 1: forearm positioned on the C-arm machine for manipulation; and (b) harvesting the great saphenous vein for graft
Fig 5: Severed upper arm and microsurgical revascularization. (a) Pre-anastomosis and (b) hand pinking immediately after arterial reperfusion.
A 5-year-old girl presented to the emergency department 5.5 h after a traumatic amputation of her right arm following a motorbike accident. The child was wearing a one-armed shirt, with the other sleeve not occupied by her arm, which became entangled in the motorbike’s wheel, causing her to be thrown to the ground and resulting in the complete amputation of her right arm. She suffered a complete transection of major neurovascular structures, fractures of the humerus and both forearm bones, along with extensive soft-tissue loss. Specifically, a transverse fracture occurred in the upper third of both forearm bones, while a spiral oblique fracture occurred in the lower third of the right humerus. The triceps brachii, biceps brachii, and brachialis muscles were torn and avulsed in an irregular manner. The radial, ulnar, and median nerves were completely contused, and the brachial artery, along with the major venous structures of the arm, was completely severed. Significant amounts of dirt and sand were embedded within the wound. The case required meticulous planning to optimize replantation success within the limited ischemic time frame.
To maximize efficiency, three surgical teams operated concurrently in two separate rooms. One team performed debridement and fracture fixation using intramedullary K-wires 1.8 mm, another team prepared vascular grafts, and the third focused on revascularization and nerve repair. We conducted a soft-tissue evaluation and observed that after debridement, the muscles retained a pink color and responded to muscle contraction with thermal stimulation. There were no signs of complete tissue damage, and after flushing the vascular lumen post-debridement, the endothelium appeared smooth and pink. Therefore, we decided to proceed with vascular revascularization with shortening and complete grafting. The nerves were severed and crushed, requiring debridement of the radial, ulnar, and median nerve stumps, followed by microsurgical repair using epineural and fascicular techniques with 8.0 nylon sutures. We sutured the muscle with Vicryl 1.0 sutures and the tendon core with nylon 3.0 sutures. Despite successful arterial and venous anastomoses, the 1st post-operative day presented a major challenge: Significant bleeding at the intramedullary nail entry point, necessitating urgent re-exploration. Careful hemostasis was achieved without compromising revascularization, demonstrating the delicate balance required in pediatric microsurgical procedures.
We administered Unasyn 1.5 g intravenously at a dose of 200 mg/kg body weight/day, with intravenous injections every 6 h, in combination with gentamicin 0.08 g at a dose of 1.2 mg/kg/day, intramuscularly every 8 h. The wound condition was monitored daily, along with vital signs. A complete blood count was performed, which showed no signs of post-operative infection. Wound culture and sensitivity testing revealed continued susceptibility to Unasyn and gentamicin, so we decided to continue their use without switching to another antibiotic.
The patient was supported by the family in daily muscle strengthening exercises. We instructed the family to perform passive range-of-motion exercises for the baby’s shoulder, elbow, and hand, including simple exercises to assist with shoulder abduction and adduction, elbow flexion and extension, wrist flexion and extension, and finger movement. These exercises were to be repeated multiple times a day, with no limitation on the number of repetitions, with monthly radiographs to monitor bone healing during the first 3 months. Bone healing was confirmed to be complete, and all fixation devices were removed in the 8th month. Starting from the 3rd month post-surgery, the patient could flex and extend the elbow, and electromyography (EMG) showed recovery of the radial nerve. By the 4th month, wrist extension was possible. At the 12th month, the patient was able to flex the fingers, but thumb opposition had not yet been achieved [Video 1]. EMG at the 10th month indicated recovery of the median and ulnar nerves.
At the 12-month follow-up, the patient exhibited significant motor recovery, including wrist and finger extension [Table 1]. However, sensory restoration remained incomplete. This underscores the need for long-term follow-up and rehabilitation, which remains a challenge in pediatric microsurgery due to the geographical and economic barriers many families face.
Important!
Your post might be deleted/hidden when other users reported/flag it. Think twice with your post title/description/comments, because the content is automatically deleted/hidden by the system. If you need quick action to delete any content in this website, you can click the Report content! button below.
We apologize for the flagged problem encountered, but for your information, every post that is flagged will be assessed as to whether it needs to be deleted or published again, this is to avoid uploading prohibited content. For that, every hidden media will be published again if it does not violate the rules of this site. In addition, posts that are uploaded repeatedly will also be deleted. We would like to emphasize that if your account is found to continue flagging and down-voting posts for no reason, your account will be blocked by the system. If you think the system has mistakenly blocked your account, you can ask us to unblock your account, but it depends on the logs we check based on the mistake you made. We try to be fair to all users, so action must be taken. Any problem can directly contact us through the Feedback form. Thank you for understanding.
- Moderator